Library
Alcohol Induced Metabolic Changes- A Case Study
Case details
A 65-year-old man was admitted to the emergency department in an unconscious state. Apparently, he had become increasingly depressed after the death of his younger son two months ago. Previously, before his death, he had been a moderate drinker, but consumption of alcohol had increased markedly over the last few weeks. He had also been eating poorly,
His elder son had dropped around to see him on Sunday morning and found him unconscious on the living room couch with two empty bottles of whiskey. Three more bottles were also found on the living room table.
On examination, he could not be roused, and his breathing was deep and noisy,
Alcohol could be smelt in his breath, and his temp was 36.6° C.
Lab findings:
Blood alcohol 550 mg/dl
Blood glucose 50mg/dl
Blood lactate 8 mmol/L
pH 7.21
What is the biochemical basis for all the laboratory findings in this patient?
Case Discussion
This is a case of Alcohol (Blood alcohol-550mg/dL) induced hypoglycemia (Low glucose-50 mg/dl) and metabolic acidosis. Metabolic acidosis, apparent from low pH (7.21), is due to underlying lactic acidosis (Blood Lactate-8mmol/L).
Alcohol-related hypoglycemia is due to hepatic glycogen depletion combined with alcohol-mediated inhibition of Gluconeogenesis. It is very common in malnourished alcohol abusers but can occur in anyone who is unable to ingest food after an acute alcoholic episode followed by gastritis and vomiting.
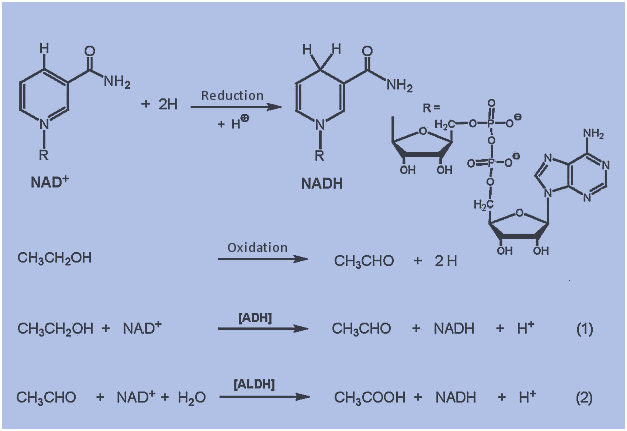
The primary pathway for alcohol metabolism involves alcohol dehydrogenase (ADH), a cytosolic enzyme that catalyzes the conversion of alcohol to acetaldehyde. This enzyme is located mainly in the liver, but small amounts are found in other organs, such as the brain and stomach.
During the conversion of ethanol by ADH to acetaldehyde, the hydrogen ion is transferred from alcohol to the cofactor nicotinamide adenine dinucleotide (NAD+) to form NADH. (Figure- Step-1)
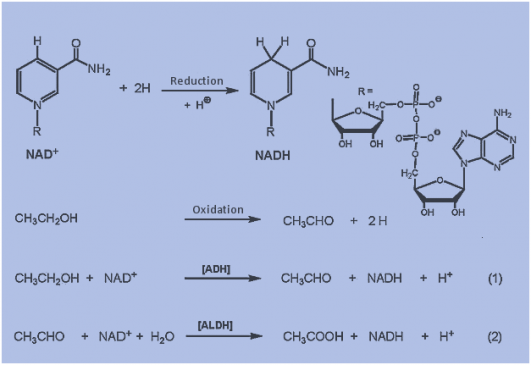
Much of the acetaldehyde formed from alcohol is oxidized in the liver in a reaction catalyzed by mitochondrial NAD-dependent aldehyde dehydrogenase (ALDH) (Figure Step 2).
The product of this reaction is acetate, which can be further metabolized to CO2 and water or used to form acetyl-CoA. As a net result, alcohol oxidation generates an excess of reducing equivalents in the liver, chiefly as NADH. The excess NADH production appears to contribute to the metabolic disorders that accompany chronic alcoholism.
1) The NADH produced in the cytosol by ADH must be reduced back to NAD+ via either the malate-aspartate shuttle or the glycerol-phosphate shuttle. Thus, the ability of an individual to metabolize ethanol is dependent upon the capacity of hepatocytes to carry out either of these two shuttles, which in turn is affected by the rate of the TCA cycle in the mitochondria, whose rate of function is being impacted by the NADH produced by the ALDH reaction.
2) The reduction in NAD+ impairs the flux of glucose through glycolysis at the glyceraldehyde-3-phosphate dehydrogenase reaction, thereby limiting energy production.
3) Additionally, there is an increased rate of hepatic lactate production due to the effect of increased NADH on the direction of the hepatic lactate dehydrogenase (LDH) reaction. This reversal of the LDH reaction in hepatocytes diverts Pyruvate from Gluconeogenesis, reducing the liver’s capacity to deliver glucose to the blood.
4) Similar to lactate formation, Malate is also produced from Oxaloacetate. The deficiency of oxaloacetate negatively affects gluconeogenesis and the functioning of the TCA cycle.
5) In addition to the negative effects of the altered NADH/NAD+ ratio on hepatic Gluconeogenesis, fatty acid oxidation is also reduced as this process requires NAD+ as a cofactor.
6) In fact, the opposite is true; fatty acid synthesis is increased, and there is an increase in triglyceride production by the liver. In the mitochondria, the production of acetate from acetaldehyde leads to increased levels of acetyl-CoA. Since the increased generation of NADH also reduces the activity of the TCA cycle, acetyl-CoA is diverted to fatty acid synthesis.
7) The reduction in cytosolic NAD+ leads to reduced activity of glycerol-3-phosphate dehydrogenase (in the glycerol 3-phosphate to DHAP direction), resulting in increased levels of glycerol 3-phosphate, which is the backbone for the synthesis of the triglycerides. Both of these two events lead to fatty acid deposition in the liver leading to fatty liver syndrome.
8) Increased [lactate]/[Pyruvate] ratio, results in hyper lactic acidemia. Lactate accumulation causes lactic acidosis (Metabolic acidosis).
9) Lactate competes with uric acid for excretion, decreasing its excretion and thus aggravating gout. Gout is a common finding in chronic alcoholics.
Leave a Reply
You must be logged in to post a comment.