Library
Image challenge-1- Answer

Case discussion
The patient is suffering from multiple myeloma.
Multiple myelomas represent a malignant proliferation of plasma cells derived from a single clone. The plasma cells in a normal individual are end-stage cells that secrete specific antibodies for a few days and then die. In contrast, the plasma cells in an individual with multiple myeloma have escaped normal control over their life span and proliferation and are not end-stage cells; rather, they divide over and over unregulated without requiring any activation by any antigen to induce proliferation. Although such a plasma cell, called a myeloma cell, has been transformed, its protein-synthesizing machinery and secretory functions are not altered; thus, the cells continue to secrete specific antibodies. The tumor, its products, and the host response to it result in a number of organ dysfunctions and symptoms of bone pain or fracture, renal failure, susceptibility to infection, anemia, hypercalcemia, and occasionally clotting abnormalities, neurological symptoms, and manifestations of hyperviscosity.
Clinical features
- Bone pain is the most common symptom of myeloma, affecting nearly 70% of patients. The lumbar spine is one of the most common sites of pain.
- Pathologic fractures are very common in multiple myeloma; 93% of patients have more than one site of bony involvement. A severe bony event is a common presenting issue.
- Spinal cord compression- This complication occurs in approximately 10-20% of patients with multiple myeloma at some time during the course of the disease.
The symptoms that should alert physicians to consider spinal cord compression are back pain, weakness, numbness, or dysesthesias in the extremities. It is common for spinal cord compressions in multiple myeloma to occur at multiple levels, so a comprehensive evaluation of the spine is warranted.
- There is an increased susceptibility to bacterial infections.
- Renal failure occurs in nearly 25% of patients. Many factors contribute to this. Hypercalcemia is the most common cause of renal failure. Confusion, somnolence, bone pain, constipation, nausea, and thirst are the presenting symptoms of hypercalcemia.
- Anemia occurs in ~80% of patients. It is usually normocytic and normochromic and related both to the replacement of normal marrow by expanding tumor cells and to the inhibition of hematopoiesis by factors made by the tumor. In addition, mild hemolysis may contribute to the anemia. A larger than expected fraction of patients may have Megaloblastic anemia due to either Folate or vitamin B12 deficiency.
- Clotting abnormalities may be seen due to the failure of antibody-coated platelets to function properly. Occasionally, a patient may come to medical attention for bleeding resulting from thrombocytopenia.
- Besides these, neurological symptoms are also seen in some of the patients. Carpal tunnel syndrome is a common complication of myeloma. Meningitis (especially that resulting from pneumococcal or meningococcal infection) is more common in patients with multiple myeloma. Some peripheral neuropathies have been attributed to multiple myeloma.
- Total Ig content may be very high, but useful antibodies are low, so the general immunity is low, and the susceptibility to infections is increased. About 53% of cases have IgG, and 25% have IgA paraproteins. However, the IgD variety, comprising about 2% of myeloma, has a poor prognosis, with survival only for about 1 year. 20% of the patients have only light-chain Immunoglobulins in serum and urine. Abnormal humoral immunity and leukopenia may lead to infection.
- Hyperviscosity- Epistaxis may be a presenting symptom of multiple myeloma with a high tumor volume. Occasionally, patients may have such a high volume of monoclonal protein that their blood viscosity increases, resulting in complications such as stroke, myocardial ischemia, or infarction. Patients may report headaches and somnolence, and they may bruise easily and have hazy vision. Patients with multiple myeloma typically experience these symptoms when their serum viscosity is greater than 4 times that of normal serum.
Diagnosis
The classic triad of multiple myeloma is marrow plasmacytosis (>10%), lytic bone lesions, and serum and/or urine M component. The confirmation of the diagnosis is done as follows-
1) Electrophoresis- The Igs of the same type (Mono Clonal antibodies) are produced in large amounts. This is seen in electrophoresis as the Myeloma band or M band with a sharp spike (Figure 1).
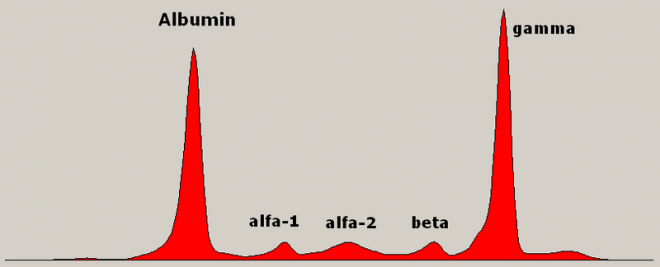
Figure 1- Serum electrophoresis showing monoclonal gammopathy (paraprotein, M-peak) in a patient with multiple myeloma
2) Bone Marrow Examination- reveals a large number of malignant plasma cells.
3) X-ray shows punched-out lesions (Figure 2).

Figure 2- Radiograph of skull showing punched-out lesions
4) Hypercalcemia and hypercalciuria are present.
5) Proteinuria is essentially present. In 20-50% of patients of multiple myeloma. Bence-Jones proteins are excreted in the urine.
6) Beta-2 microglobulin- The level of beta-2 microglobulin is increased in patients with renal insufficiency without multiple myeloma, which is one reason that it is a useful prognosticator in multiple myeloma. The prognosis of patients with multiple myeloma and impaired renal function is reduced.
7) Histologic Findings- In patients with multiple myeloma, plasma cells proliferate within the bone marrow.
Treatment
Chemotherapy and local irradiation are undertaken.
Prognosis
It is generally good, and the average survival is more than 5 years. The major causes of death are progressive myeloma, renal failure, sepsis, or therapy-related acute leukemia. Nearly a quarter of patients die of myocardial infarction, chronic lung disease, diabetes, or stroke. All intercurrent illnesses are related more to the age of the patient group than to the tumor.
Leave a Reply
You must be logged in to post a comment.